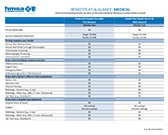
Quick view of all plan benefits
Benefits shown are for services received from an in-network provider.
|
Preferred Provider Plan PPO with Prescription Drug, Vision and Complementary Care |
|---|
|
Annual deductible |
|
Annual Out-of-pocket Maximum $2,500 per person |
| Annual Preventive Health Evaluation: $10 Office Visits: $10 You pay 10% for these services:
$10 |
| Preferred Provider Plan PPO Plan documents |
|
Health Plan Hawaii Plus HMO with Prescription Drug, Vision and Complementary Care |
|---|
|
Annual deductible |
|
Annual Out-of-pocket Maximum $1,500 per person |
| Annual Preventive Health Evaluation: $0 Office Visits: $12 You pay $0 for these services:
$25 Hospital Room and Board: $0 copayment per day |
| Health Plan Hawaii Plus HMO Plan documents |
with Prescription Drug, Vision and Complementary Care
$2,500 per person
$7,500 (max) per family
with Prescription Drug, Vision and Complementary Care